Download the alternative format
|
Questionnaire Background for Interviewer |
|
This questionnaire is designed to collect comprehensive information on possible risk factors for hepatitis A. It is designed for cluster/outbreak investigations where the source of infection is unknown, but the questionnaire could be applied to investigate sporadic cases. Data captured: – Case demographics – Other risk factors – Clinical information – Food exposures – Laboratory information Since outbreaks of hepatitis A are often linked back to contaminated food products, please collect as much details as possible for each item, including restaurant exposures. Also consider using a calendar to probe. The questionnaire is estimated to take approximately 1 hour to complete |
|
FOR LOCAL USE ONLY – PLEASE REMOVE THIS PAGE IF SENDING TO PHAC | |
|
i. Case Information | |
|
Case Name: |
Proxy Name: |
|
Health Card Number: _____________________________________ |
|
|
Street Address: ______________________________ City/Town: ______________________________ Postal Code: ______________________________ |
Home phone: ______________________________ Work phone: ______________________________ Cell Phone: ______________________________ |
|
Physician: |
Physician Phone: |
|
Occupation: |
Place(s) of employment: |
|
ii. Symptoms | |
|
Asymptomatic: ☐ Y ☐ N ☐ DK If yes, reason case was tested: ☐ Reported risk factors, specify: ☐ No risk factors ☐ Other | |
|
Symptoms: Jaundice ☐ Y ☐ N ☐ DK If yes, date of jaundice onset: d____ / m____ / y______ Abdominal pain ☐ Y ☐ N ☐ DK Fatigue ☐ Y ☐ N ☐ DK Dark Urine ☐ Y ☐ N ☐ DK Vomiting ☐ Y ☐ N ☐ DK Anorexia ☐ Y ☐ N ☐ DK Fever ☐ Y ☐ N ☐ DK Pale Stool ☐ Y ☐ N ☐ DK Elevated liver enzymes ☐ Y ☐ N ☐ DK Other: ☐ Y ☐ N ☐ DK If other, please specify: | |
|
Underlying conditions or medications that suppress the immune system (e.g. pregnancy, diabetes, cancer, steroids)? ☐ Y ☐ N ☐ DK If yes, please specify: | |
|
iii. Ill Contacts | |
|
Were any of (your/case’s) contacts ill with similar symptoms in the 7 days before (you/case) became ill? ☐ Y ☐ N ☐ DK If yes, can you tell me who? *Contacts include household members, sexual partners, individuals who prepared food for (you/case), children or adults that (you/case) assisted with bathroom use or diaper change, or other individuals with whom (you/case) may have come into contact with their vomit and/or stool | |
|
Name:___________________________________________ Gender: Phone Number: ___________________________ Relationship to case:________________________________ Age: ________ | |
|
Name:___________________________________________ Gender Phone Number: ___________________________ Relationship to case:________________________________ Age: ________ | |
|
Name:___________________________________________ Gender Phone Number: ___________________________ Relationship to case:________________________________ Age: ________ | |
Section 1. Case information
|
Case interviewed by: |
Date of interview: d____/m____/y____ |
|
Health Unit/Authority: |
Date reported to Health Unit/Authority: d____/m____/y____ |
|
Province/Territory: | |
|
Respondent was: ▢ Case ▢ Parent ▢ Spouse ▢ Caretaker ▢ Other, specify: | |
|
Gender: ☐ M ☐ F ☐ Another Gender ☐ Not asked/Unknown |
Age: _________ |
Section 2. Clinical information
Section 2. Clinical Information | |||||
|
To be filled out by interviewer |
Date of first positive specimen collection: d_____ / m______ / y______ |
Anti-HAV IgM:_______________________ ☐ Positive ☐ Indeterminate | |||
|
Specimen submitted for genotyping ☐ Y ☐ N ☐ DK |
If yes, specify genotype: | ||||
|
Asymptomatic: ☐ Y ☐ N ☐ DK If no, date of first symptom onset: d_______ / m_______ / y______ |
Date of onset of jaundice: d_______ / m_______ / y______ | ||||
|
Admitted* to hospital because of the illness? ☐ Y ☐ N ☐ DK *Do not include individuals who visit an emergency room or outpatient clinic |
Date of admission: d______ / m______ / y______ Date of discharge: d______ / m______ / y______ ☐ Still hospitalized | ||||
|
Have you been diagnosed with hepatitis A in the past? ☐ Y ☐ N ☐ DK If yes, date: d_______ / m_______ / y______ |
Have you received hepatitis A vaccine in the past? ☐ Y ☐ N ☐ DK If yes, date: d_______ / m_______ / y______ # of doses: | ||||
|
Have you received immunoglobulin in the past 5 months? ☐ Y ☐ N ☐ DK If yes, date: d______ / m______ / y_______ | |||||
|
To be filled out by interviewer |
Case deceased? ☐ Y ☐ N Date of Death: d______ / m______ / y______ If yes, was Hepatitis A infection the underlying/contributing cause of death? ☐ Y ☐ N ☐ DK If yes, was determination based on death certificate? ☐ Y ☐ N ☐ DK | ||||
|
Section 3: Exposure and Infectious Period |
|
Enter symptom onset date, using this as day 0, then count back to determine the exposure period. In absence of a symptom onset date and for asymptomatic cases, please use, in order of preference, (i) specimen collection date, or (ii) lab reporting date, to calculate incubation and infectious periods as the symptom onset date. 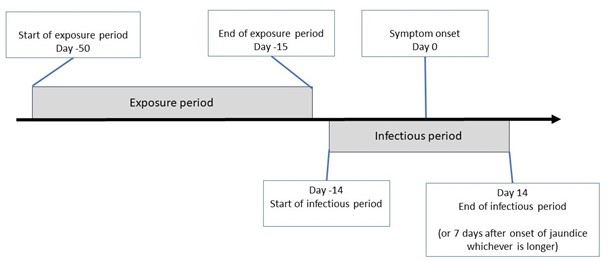 |
|
Section 4: Travel Information |
|
In the 50 to 15 days before onset of illness, that is from d____/m_____/y_____ through d____/m____/y____, did (you/case) travel within or outside of Canada? ☐ Y ☐ N ☐ DK |
|
If yes: ☐ Within Province/Territory ☐ Other Province(s)/Territory(ies) ☐ Outside Canada |
|
Specify travel destination(s) (country/town/resort): |
|
Departure: d____ / m____ / y______ Return: d____ / m____ / y______ |
|
Section 5. Risk Factors | ||
|
I’d like to ask you about some common risk factors for acquiring Hepatitis A. In the 50-15 days before onset of illness did (you/case): **Please record any potential close contacts in section iii | ||
|
Contact with a known hepatitis A case: ☐ Y ☐ N ☐ DK |
Contact with a jaundiced individual: ☐ Y ☐ N ☐ DK | |
|
Consume a meal or food product that was handled by someone who was ill? ☐ Y ☐ N ☐ DK | ||
|
Live in a residential institution? ☐ Y ☐ N ☐ DK (e.g. Nursing home, long term care facility, prison, dormitory or boarding school) |
Name/location/dates: | |
|
Attend a day care or day facility ? ☐ Y ☐ N ☐ DK (e.g. child or adult) |
Name/location/dates : | |
|
Work/volunteer at a daycare or residential institution or Hospital/Health Care |
Name/location/dates : | |
|
Diaper a child or assist a child or adult with bathroom use? ☐ Y ☐ N ☐ DK | ||
|
Receive a blood transfusion or blood products during the incubation period? ☐ Y ☐ N ☐ DK If yes, date: d______ / m______ / y__________ |
Receive an organ transplant during the incubation period? ☐ Y ☐ N ☐ DK If yes, date: d______ / m______ / y__________ | |
|
Donate blood during the incubation period? ☐ Y ☐ N ☐ DK If yes, date: d______ / m______ / y__________ | ||
|
Use the following sources of drinking water? (check all that apply) ☐ Municipal ☐ Well/Private water source ☐ Bottled water, specify: _______________ ☐ Other, specify: _______________ | ||
|
Swim in/go into the ocean, a lake, a river, a pool or a hot tub? ☐ Y ☐ N ☐ DK If yes, specify type of water source and location: | ||
|
Did (you/case) come in contact with, or were (you/case) exposed to, sewage back-up? ☐ Y ☐ N ☐ DK If yes, please specify: | ||
|
Were you homeless, That is were you living on the street, in a shelter, in a single room occupancy hotel, in a car or couch surfing? ☐ Y ☐ N ☐ Prefer not to answer ☐ DK | ||
|
Section 6. Sexual and Drug Activity: Skip this section if the case has already been asked |
|
INTSRUCTIONS FOR INTERVIEWER: Please ask these questions to male and female adult cases (>18 years) |
|
Were (you/case) currently sexually active in the 50-15 days prior to symptom onset? ☐ Y ☐ N ☐ Refuse |
|
If yes, Have (you/case) engaged in oral-anal sexual contact in the past 50 -15 days? ☐ Y ☐ N ☐ Refuse |
|
Did (you/case) use intravenous drugs in the 50-15 days prior to symptom onset? ☐ Y ☐ N ☐ Refuse |
|
Did (you/case) use non-intravenous drugs in the 50-15 days prior to symptom onset? ☐ Y ☐ N ☐ Refuse |
|
Section 7. Special Diets or Food Preferences |
|
First I would like to ask some general questions about (your diet/case’s) diet and food preferences. |
|
Are (you/case) a vegetarian? ☐ Y ☐ N ☐ DK If yes, do (you/case) ever eat: Eggs ☐ Y ☐ N ☐ DK Dairy ☐ Y ☐ N ☐ DK Fish ☐ Y ☐ N ☐ DK Poultry ☐ Y ☐ N ☐ DK Red meat ☐ Y ☐ N ☐ DK Other Meat ☐ Y ☐ N ☐ DK If yes, specify: ________________ |
|
Are (you/case) allergic to any foods ? ☐ Y ☐ N ☐ DK If yes, specify which foods: |
|
Are there any foods/food groups that (you/case) never eat? ☐ Y ☐ N ☐ DK If yes, describe: |
|
In the 50 – 15 days prior to illness, were (you/case): On a special or restricted diet? (e.g. raw food diet, vegan, diabetic diet, kosher, halal) ☐ Y ☐ N ☐ DK If yes, describe: ____________________________________________________________________________ Taking a dietary or nutritional supplement? (e.g. meal replacements, protein powder, vitamins, herbs, kratom) ☐ Y ☐ N ☐ DK If yes, describe (include purchase location): _____________________________________________________ Did you consume any bottled, pre-made health drinks? (e.g. Kombucha, coconut water) ☐ Y ☐ N ☐ DK If yes, describe (include purchase location): _______________________________________________________ |
|
Section 8. Food eaten outside the home | |||
|
In the 50-15 days prior to illness onset did (you/case) eat food outside home at a social gathering or at any of the following food establishments? (including food taken from a restaurant and eaten at home and samples eaten at establishments such as grocery stores)? | |||
|
Type of Gathering/Establishment Name(s): |
Details of food(s) eaten | ||
|
Social gathering or event (e.g. family or friends house, snacks at work, conferences, wedding or parties) ☐ Y ☐ N ☐ DK If yes, are you aware of anyone else who became ill with diarrhea following the gathering? ☐ Y ☐ N ☐ DK If yes, number ill? ______ |
Event name/description:
Location:
Date of gathering: d______ / m______ / y______
Number attended: |
| |
|
Did you eat any fast food or at other restaurants? This could include food or drinks from a coffee shop, cafeteria, street vendor, concession stand or convenience stores. Also list any samples from a grocery store. | |||
|
Food Establishment Name |
Address/Location |
Dates(s) |
Food ordered/Eaten |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Additional details from above-listed food establishments: | |||
|
| |||
|
Section 9. Home Food Purchase: | ||
|
Where do (you/case) usually purchase food for home consumption? This includes grocery stores, farmers markets, specialty stores, food banks, or online purchases such as Amazon, Well.ca or other e-commerce. Collecting receipts, purchase data or loyalty cards if available can be helpful given the long incubation period. Consent form for collecting loyalty card information is available from your provincial/territorial health authority or PHAC | ||
|
A
|
Store/website name:
Location: |
Purchased food online (delivery or curbside pick-up) ☐ Y ☐ N ☐ Unknown Are receipts, invoices, email notifications available? ☐ Y ☐ N Loyalty Card? ☐ Y ☐ N ☐ Unknown Would you be willing to share your loyalty card number and purchase information with us? ☐ Y ☐ N |
|
B
|
Store/website name:
Location: |
Purchased food online (delivery or curbside pick-up) ☐ Y ☐ N ☐ Unknown Are receipts, invoices, email notifications available? ☐ Y ☐ N Loyalty Card? ☐ Y ☐ N ☐ Unknown Would you be willing to share your loyalty card number and purchase information with us? ☐ Y ☐ N |
|
C
|
Store/website name:
Location: |
Purchased food online (delivery or curbside pick-up) ☐ Y ☐ N ☐ Unknown Are receipts, invoices, email notifications available? ☐ Y ☐ N Loyalty Card? ☐ Y ☐ N ☐ Unknown Would you be willing to share your loyalty card number and purchase information with us? ☐ Y ☐ N |
|
D
|
Store/website name:
Location: |
Purchased food online (delivery or curbside pick-up) ☐ Y ☐ N ☐ Unknown Are receipts, invoices, email notifications available? ☐ Y ☐ N Loyalty Card? ☐ Y ☐ N ☐ Unknown Would you be willing to share your loyalty card number and purchase information with us? ☐ Y ☐ N |
|
Additional details from above-listed stores. If applicable, include information on typical purchases from specialty/online stores, details on purchase method, and if the case is willing to share receipts, invoices, etc. | ||
|
| ||
|
Section 10. Meal Delivery Kit Purchase: | |
|
In the 50-15 days prior to illness onset did (you/case) consume food prepared from a meal delivery kit (e.g., Goodfood, Hello Fresh, Chef’s Plate, Red Apron, etc.)? ☐ Yes ☐ Probably ☐ No If yes please provide details below. | |
|
Purchase Information: |
Meal names, consumption dates, ingredients and substitutions: |
|
Name of company: Date of delivery: Are receipts, invoices, email notifications, or recipe cards available? ☐ Y ☐ N ☐ Unknown |
|
|
Section 11: Food Exposures |
|
INSTRUCTIONS TO READ TO CASE I am interested in the food you ate during the 50-15 days before your illness onset date; that is from d____/m_____/y_____ through d____/m____/y____. For each food item please give me your best guess as to whether you ate the food, you’re not sure but you probably ate the food, or you did not eat the food. Please include food eaten on their own, or as part of a salad, sandwich, or dish.
INSTRUCTIONS FOR INTERVIEWER For each food item that the case consumed ask follow up questions regarding the brand, location of purchase. Please select an answer for each question or indicate if question not asked Yes – indicates case ate the food DK – indicates case doesn’t know if they ate the food Prob. – indicates the case probably ate the food No – indicates case did not eat the food |
|
|
Yes |
Prob |
No |
DK |
IMPORTANT. Please complete in as much detail as possible Type / Variety / Brand |
Where purchased or eaten: Specify grocery store or restaurant name |
|
VEGETABLES Include raw or cooked vegetables (exclude vegetables purchased canned) | ||||||
|
Any tomatoes, including any in a dish or meal such as a salad, sandwich, burger or taco If yes, were they: |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Cherry or grape |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Semi-dried ☐ packed in oil ☐ loose |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Sun-dried ☐ packed in oil ☐ loose |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Any lettuce or leafy greens, including in a dish or meal such as a salad, sandwich, burger or taco If yes, please specify type(s) below: |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Iceberg ☐ prepackaged ☐ loose/head |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Romaine ☐ prepackaged ☐ loose/head |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Spinach ☐ prepackaged ☐ loose |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Mesclun lettuce/spring mix ☐ prepackaged ☐ loose |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Kale ☐ prepackaged ☐ loose |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Arugula ☐ prepackaged ☐ loose |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Other lettuce/leafy greens If yes, specify: ___________________ ☐ prepackaged o loose/head |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Any commercially pre-packaged salad kits (e.g. in a bag or container, may include dressing, toppings), excluding prepared or ready to eat salads If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Any store-bought prepared or ready to eat green salads (e.g. prepared Caesar, kale, garden, chef’s spinach) If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Store-bought potato salad |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Store-bought pasta salad |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Store-bought other salad (e.g. Greek, quinoa, bean) |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Any cabbage (e.g. whole, shredded cabbage, coleslaw) ☐ prepackaged ☐ loose/head |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Coleslaw ☐ prepackaged ☐ homemade |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Any microgreens or sprouts including in a dish or meal such as on a sandwich or salad (e.g. bean or alfalfa sprouts, broccoli microgreens) If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Cucumbers ☐ English ☐ Field ☐ Mini |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Bell peppers (e.g. red, green, yellow peppers) If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Hot peppers (e.g. jalapeno, serrano, habanero) If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Celery |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Carrots (not mini) |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Mini/baby carrots |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Peas (fresh, raw pea pods, snap peas, snow peas) |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Green or yellow beans |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Broccoli |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Cauliflower |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Onions If yes, please specify type(s) below: |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
White/yellow onions |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Green onions |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Red onions |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Other onions If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Leeks |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Mushrooms |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Other vegetables If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Frozen vegetables |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Vegetable juices (e.g. tomato juice, carrot juice) If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
HERBS AND SPICES Include fresh herbs and spices (exclude dried herbs and spices) | ||||||
|
Fresh basil ☐ Thai ☐ Conventional |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Fresh cilantro/coriander |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Fresh parsley |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Other fresh herbs (e.g. oregano, dill, mint, rosemary, chives, thyme) If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
FRUIT Include raw or cooked fruits (exclude fruits purchased canned) | ||||||
|
Fruit salad/pre-cut fruit or fruit platter |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Melon If yes, please specify type(s) below: |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Cantaloupe ☐ Fresh ☐ Frozen |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Honeydew melon ☐ Fresh ☐ Frozen |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Watermelon ☐ Fresh ☐ Frozen |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Other melons If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Apples |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Pears |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Peaches ☐ Fresh ☐ Frozen |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Nectarines ☐ Fresh ☐ Frozen |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Apricots |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Plums |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Citrus fruits (e.g. oranges, grapefruit, lemons, limes) If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Berries If yes, please specify type(s) below: |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Strawberries ☐ Fresh ☐ Frozen ☐ Dried |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Raspberries ☐ Fresh ☐ Frozen ☐ Dried |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Blueberries ☐ Fresh ☐ Frozen ☐ Dried |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Blackberries ☐ Fresh ☐ Frozen ☐ Dried |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Other berries (e.g. cranberries, gooseberries, tayberries) If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Bag of mixed frozen fruit or berries |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Cherries |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Grapes |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Bananas |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Mangos ☐ Fresh ☐ Frozen ☐ Dried |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Papaya ☐ Fresh ☐ Frozen ☐ Dried |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Kiwi |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Pomegranate ☐ Fresh (including ready-to-eat seeds) ☐ Frozen |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Pineapple |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Coconut ☐ Fresh ☐ Frozen ☐ Dried/shredded |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Avocado (including guacamole) ☐ Fresh ☐ Frozen |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Olives |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Other fruit If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Unpasteurized apple cider or fruit juice If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Smoothies made with fresh or frozen fruit or produce, made at home or purchased fresh-made from a store, restaurant, or café |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Bottled, pre-made smoothie |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
FISH AND SEAFOOD | ||||||
|
Any fish (including fresh, canned, jarred, frozen) If yes, please specify type(s) below |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Smoked fish (e.g. smoked salmon) If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Fish – eaten raw (e.g. sushi, tartare, sashimi, ceviche) If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Other fish (e.g. fresh, frozen, cooked, dried) If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Any Shellfish If yes, please specify type(s) below |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Mussels If yes, was it eaten raw oY oN oDK |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Clams If yes, was it eaten raw oY oN oDK |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Shrimp/Prawns If yes, specify:___________________ If yes, was it eaten raw oY oN oDK |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Any oysters If yes, was it eaten raw oY oN oDK |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Any other shellfish (e.g. scallops, cockles, crab, crayfish, lobster) If yes, specify:___________________ If yes, was it eaten raw oY oN oDK |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Other seafood or seaweed products If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
OTHER MEAT/ANIMAL PRODUCTS | ||||||
|
Any deli meats/cold cuts (e.g. Bologna, salami, pepperoni, turkey, ham) If yes, please specify type(s) below |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Pre-packaged deli meat If yes, specify: ___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Deli meat sliced at the deli counter If yes, specify: ___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Hot dogs or corn dogs If yes, heated before eating ☐Y ☐N ☐DK |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Dried/cured meat products (e.g. beef jerky, dried sausage, summer sausage) If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Pâté/meat spread If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Shawarma/donair/gyro |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
DAIRY and DAIRY SUBSTITUTES | ||||||
|
Unpasteurized (raw) milk If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Other unpasteruized dairy products If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
CHEESE | ||||||
|
Any cheese made with unpasteurized (raw) milk If yes, specify:___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Cheese sliced at the deli counter If yes, specify: ___________________ |
☐Y |
☐P |
☐N |
☐DK |
|
|
|
Section 12: Demographics |
|
My final question asks about your race or racial background. In our society, people are often described by their race and consider themselves to be “White” or “Black” or “South Asian”. This information is being collected to understand who is being infected with Hepatitis A to help guide our investigation. (Interviewer note: if a case is uncomfortable with answering, skip the question). |
|
Which race category best describes you? Select all that apply from the options:
☐ Black (e.g. African, Afro-Caribbean, African Canadian descent) ☐ East/Southeast Asian (e.g. Chinese, Korean, Japanese, Taiwanese, Filipino, Vietnamese, Cambodian, Thai, Indonesian, other Southeast Asian descent) ☐ Indigenous (e.g. First Nations, Inuk/Inuit, Métis descent): ☐ First Nations ☐ Inuk/Inuit ☐ Métis ☐ Latino (e.g. Latin American, Hispanic descent) ☐ Middle Eastern (e.g. Arab, Persian, West Asian descent – for example, Afghan, Egyptian, Iranian, Lebanese, Turkish, Kurdish) ☐ South Asian (e.g. South Asian descent-for example, East Indian, Pakistani, Bangladeshi, Sri Lankan, Indo-Caribbean) ☐ White (e.g. European descent) ☐ Other group, specify: _________________________ ☐ Unsure/prefer not to answer |
Notes/General Comments:
Notes: